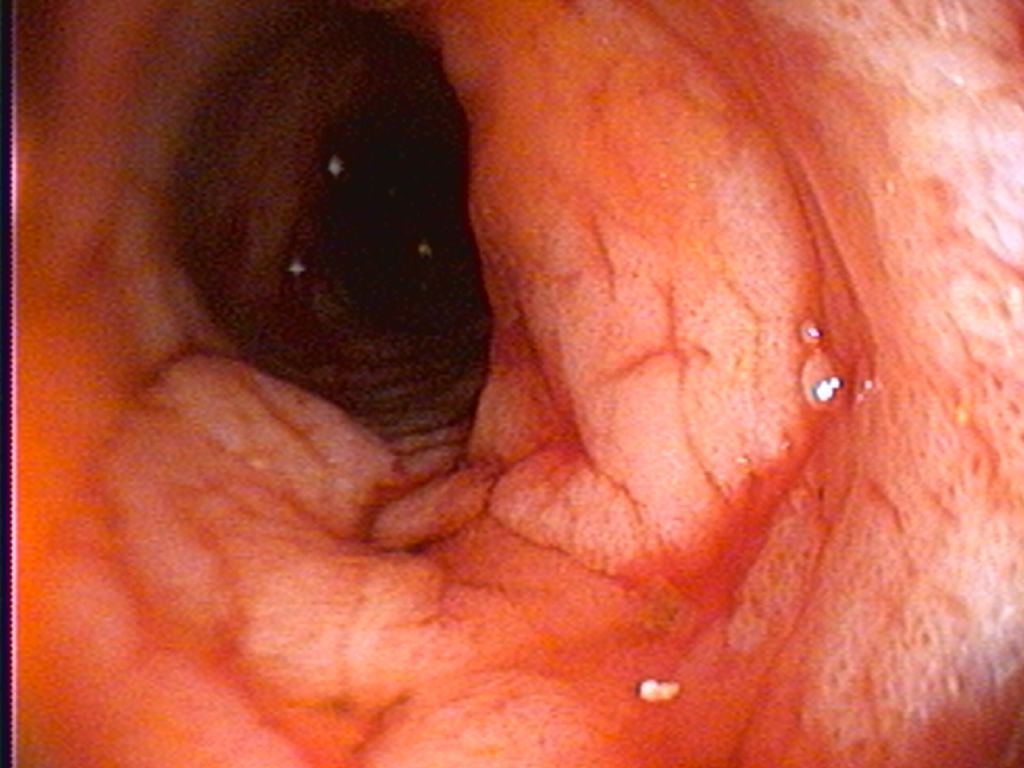
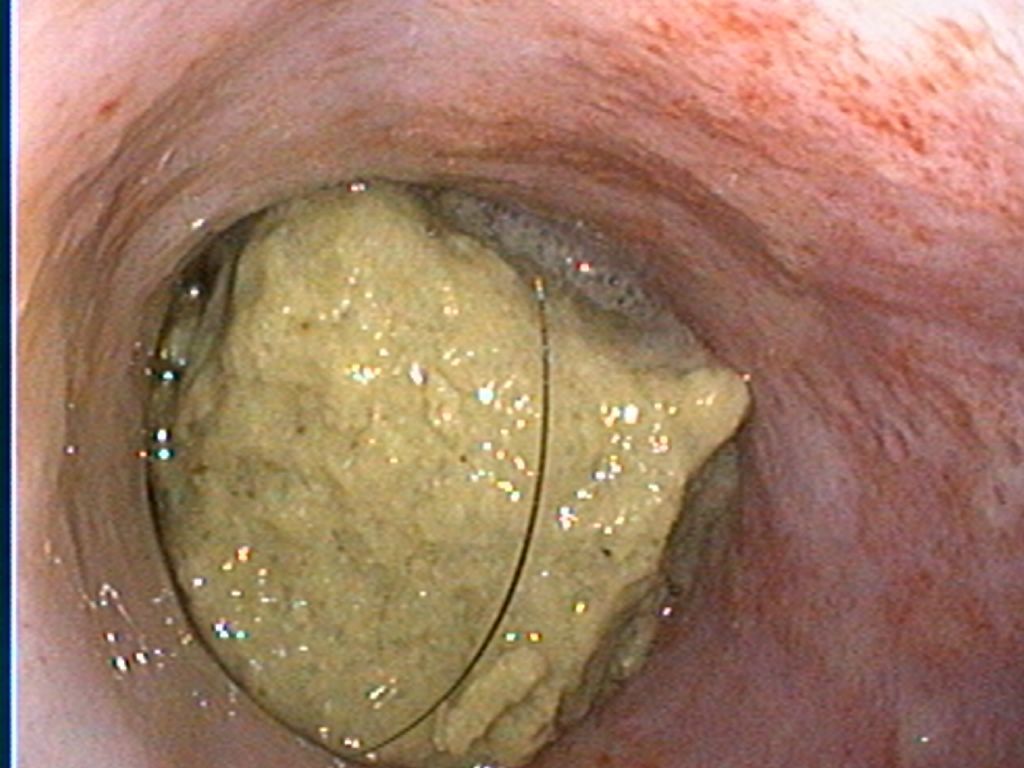
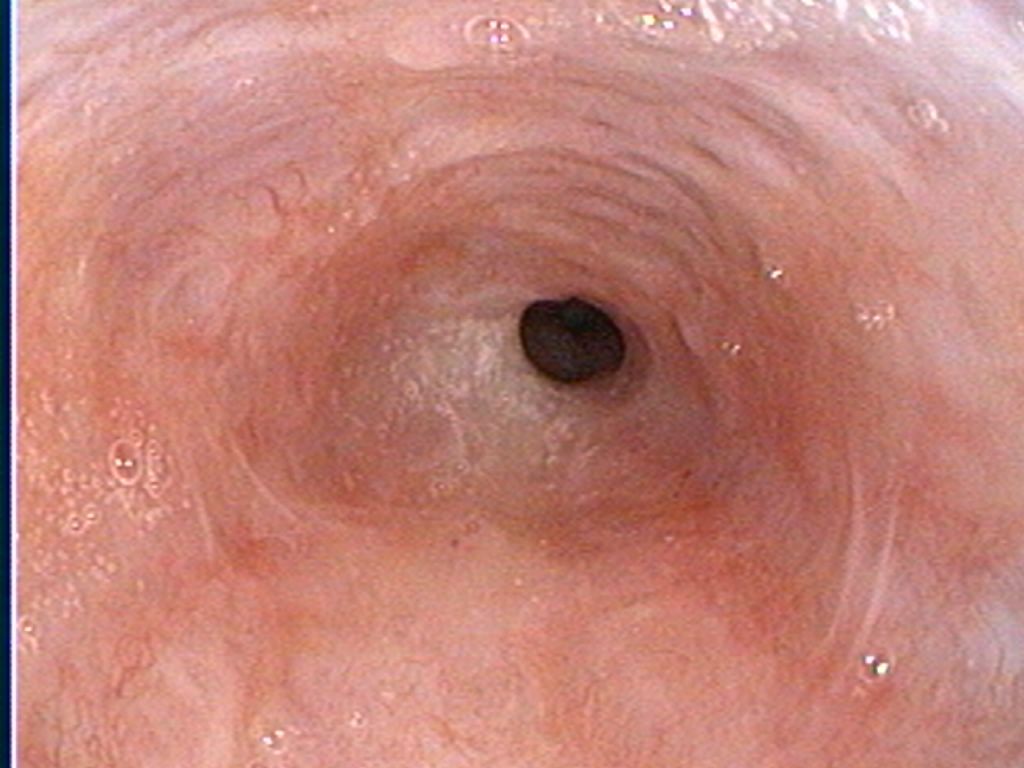
In their never ending quest to amaze pet owners and veterinarians, dogs (and sometimes cats) are always demonstrating how many things they consider "edible". While food products such as bones and corn cobs can be understood, less tempting items such as underpants, toys, stuffed animals, shoes and jewelry tend to make us scratch our heads. Most of these items will make their way down the esophagus into the stomach, and occasionally will pass through their digestive system without any major problems. However, quite often these items will become lodged somewhere and require treatment to be removed (eg: endoscopy to pull it out of the stomach or general surgery if further into the small intestine). On rare occasions a foreign object will become lodged in the esophagus and cause the pet great discomfort. Over the past while I have been asked to remove a few esophageal foreign bodies and these are never pleasant or easy to do. Objects that become lodged in the esophagus are typically larger and more firm in nature, making it harder for the pet to swallow down to the stomach. Once the object becomes stuck it can be difficult to dislodge and swift treatment is the best chance for preventing more serious secondary trauma. In particular, animals with esophageal foreign bodies are at a risk of pressure ulcerations forming in the esophagus (where the foreign material is tightly wedged). The esophagus is not able to distend like a stomach would and pressure sores (ulcers) can start to form fairly quickly. Should the foreign material be successfully removed, the esophagus begins to repair itself and scar tissue can form. If a large amount of scar tissue forms in an area there is a risk of stricture (shrinking down or narrowing of the opening in the esophagus). In extreme cases these strictures can cause the esophagus to become so narrow that food cannot get through. When this happens the process for opening that narrowed spot back up can be time consuming, uncomfortable for the pet, and expensive. In many cases, signs of an esophageal foreign body can be difficulty swallowing, repeated swallowing motions despite not currently eating anything, drooling, regurgitation when trying to eat, and even difficulty breathing if the object is putting pressure on the trachea (airway). BOTTOM LINE: If you think your pet has an object stuck in their throat, don't wait! The sooner you can get to a veterinarian to investigate the better. Case #1: 5 year old small breed dog that was eating a dental chew and swallowed a large piece that became lodged in the esophagus. She was not experiencing any respiratory issues and was stable, so the esophagoscopy was performed later that day. The foreign object was removed leaving a mild to moderate amount of inflammation to the tissue (seen as small red depressions on the lower left image. This little girl made a full recovery. Case #2: 10 year old small breed dog with history of regurgitation for a number of days prior to presentation to his veterinarian. Radiographs showed a large amount of foreign material in the esophagus and esophagoscopy was performed to attempt to remove the obstruction. During an extremely difficult procedure we removed multiple pieces of a small plastic toy combined with a large amount of hair. The esophagus was extremely ulcerated and we were concerned about a secondary stricture formation. Despite aggressive therapy a severe stricture did form and ultimately humane euthanasia was elected. While unfortunate, this serves to demonstrate the importance of recognizing a problem and treating it as quickly as possible.
At some point or another the chances are that your veterinarian has recommended running "wellness" bloodwork on your pet during a visit. While many people appreciate the benefit of wellness testing, there is still some confusion as to what it is and why we (as veterinarians) recommend it. Quite often, the question we'r
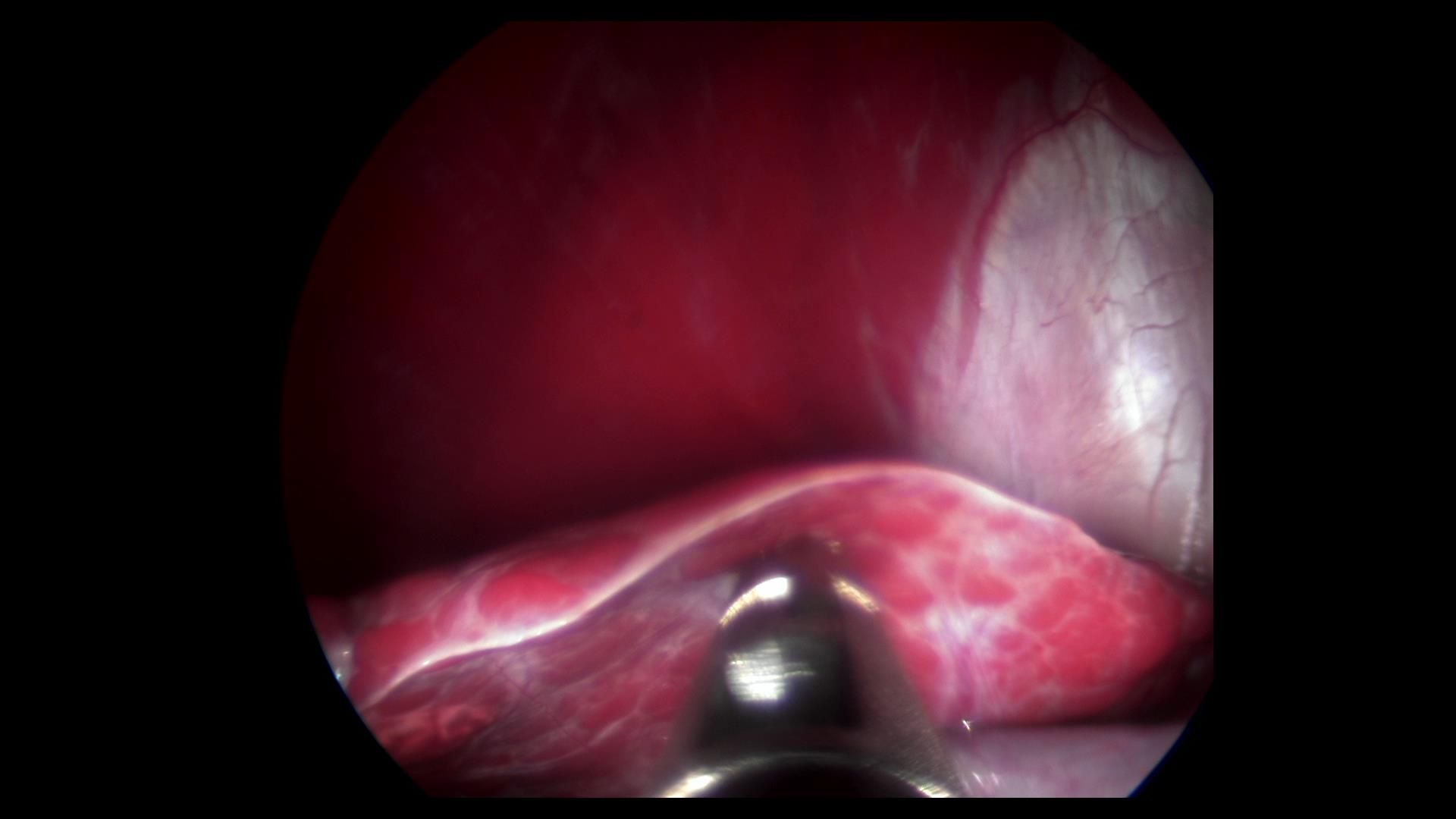
It's happened to all of us - we're in the middle of a surgery and our technician tells us that the patient is regurgitating. While we continue to operate, our techs quickly clean out the mouth and double check to ensure the endotracheal cuff is snug. Now what? There are a variety of ways to address an obvious regurgita